
Pandemic is one of my favorite board games. Four players cooperate to stop the spread of four diseases from wiping out the world. Anyone who plays with an ounce of strategy is unknowingly thinking about network effects: prioritize treating the infected cities that have more connections to other cities, target the cities with more disease cubes, or invest some early moves in discovering a cure rather than treating diseases.

Randomly shuffled into the card deck is the dreaded “Epidemic!” card that increases the infectivity rate and intensifies the spread. Through this card, Pandemic models the behavior of exponential growth that your team is racing against [1].
Today, it’s hard to imagine a scenario where four epidemics take over the world. In recent years, epidemics tend to be short-lived and small in scale [2]. The recent 2009 flu pandemic took 14,000 lives worldwide. That’s just 0.0002% of the global population. 100 years ago, the 1918 flu pandemic took around 75 million lives. 75 million! That was 3-5% of the world population.
But in the 1300s, bubonic plague or “Black Death” took out 40-60% of Europe’s population after emerging from the steppes of China. Throughout the 1500s, smallpox wiped out entire Native American tribes after they came in contact with early European settlers.

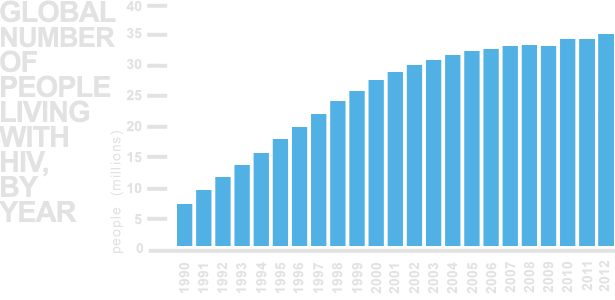
Today, we find a different type of epidemic. In the early 20th century, a hunter from a village in the southeastern rain forests of Cameroon was chopping up a chimpanzee for meat and cut himself in the process. He contracted a mutation of the chimp’s virus, which would become what is today called Human Immunodeficiency Virus, or “HIV” [3]. This virus would go on to kill 35 million people over the next 30 years while another 35 million people were HIV-positive in 2012.
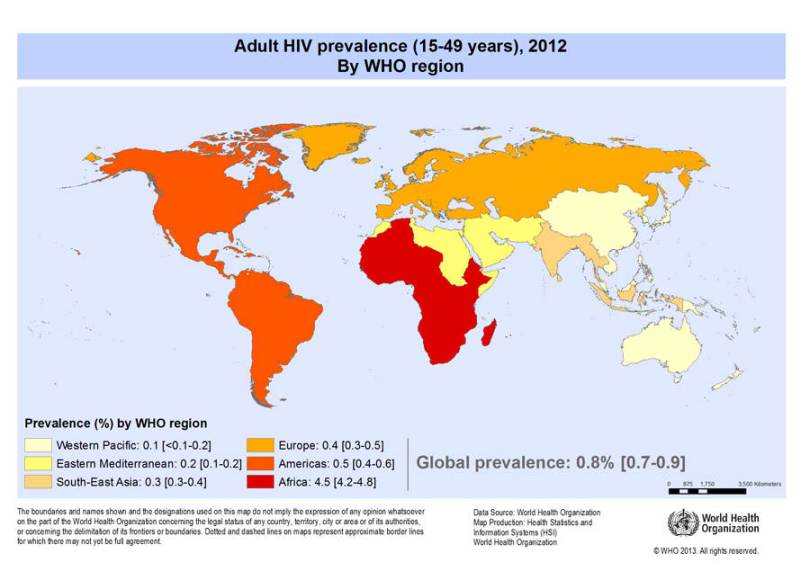
While HIV is a serious health concern, especially in African countries like Swaziland where 26% of the adult population has HIV, its growth behavior looks nothing like that of the Black Plague. So what causes these behavioral differences?
Modeling Epidemics
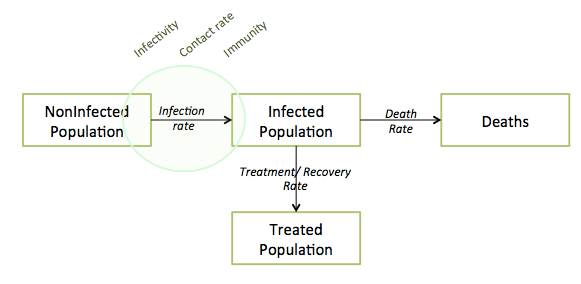
Below is a general diagram that describes the structure of all epidemics. Each box represents a number of people, and every individual in the population falls in one of these four boxes.

The above shows an important mathematical relationship – as long as the infection rate is greater than the sum of the treatment and death rates, the epidemic grows (the Infected Population increases). Furthermore, the infection rate is a function of the size of the current infected population. The more people carrying the disease today, the greater the chances of healthy people getting it – it’s a reinforcing loop. This leads to the dark realization that deaths, through decreasing the infected population, can help save healthy people from infection. If you internalize the above structure, you will understand the key dynamics of any epidemic.
Infection
So what are the key drivers of the Infection Rate?
There’s an infectivity rate – the ease at which the disease transfers when an infected body contacts a healthy body. The airborne flu has high infectivity while rabies, which requires saliva to break skin, is much lower. HIV has a similar profile, requiring bodily fluids other than saliva to contact open wounds.
Infection is also driven by the contact rate between the infected and noninfected. Society’s modernity and interconnectedness can help a disease spread – the 2013 Ebola outbreak reached Nigeria after an infected Liberian man took a flight from Liberia to Nigeria. Dense population zones like Mumbai or Shanghai make it extremely easy to transmit a flu. Social norms and individual behavior affect the types of contact made, and thus also affects the disease’s infection rate. Ebola outbreaks in African villages were intensified due to religious practices that require relatives to kiss and touch the corpse.
Populations have different susceptibility to the same disease. Some populations are naturally immune or more resistant to a disease through natural selection. When Europeans invaded the New World, they brought many diseases that destroyed a previously unexposed Native American population – measles, scarlet fever, influenza, tuberculosis, cholera, etc. Spanish Conquistador Hernando Cortes brought with his troops infectious diseases that whittled the Aztec population from 30 million to just 3 million in 5 years.
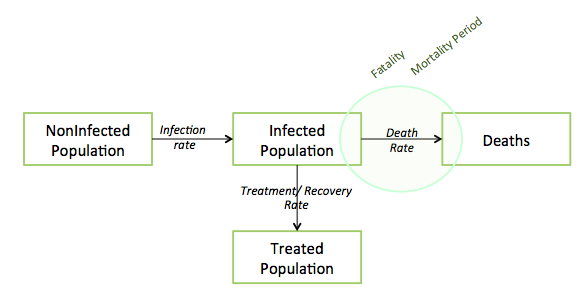
Death
After infection, the possibility of death awaits. When we hear that a disease is “deadly”, reporters are usually referring to its fatality rate – the likelihood that someone who already has the disease will die. An extreme example is rabies, which has a 100% fatality rate once symptoms appear.
The 2013 Ebola virus outbreak is a compelling modern example – the Zaire Ebola virus type has historically killed 79% of its hosts. It’s the largest Ebola outbreak to date – yet it has killed less than 1,000 people as of July 2014. In fact, more people have died from diarrhea in one day than Ebola has killed in its entire history. So a disease can be called “deadly” (high fatality rate) even though it has yet to spread on a wide scale.
Different diseases take different periods of time to kill its host, and a disease that kills quickly is actually hurting its chances at growth. Diseases must race against time, trying to keep their infected hosts alive and operative long enough for them to meet new bodies. When the rate of exit exceeds the rate of infection, the infected population collapses. The graph below marks the number of deaths from the 1918 Spanish Flu, an infamously lethal disease. Because it was so deadly and quick to kill, its hosts did not live long enough to spread the flu to a wider population, creating the rapid boom and bust cycles compressed into just 2-3 months.
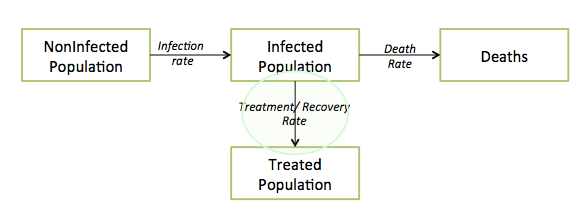
Not all diseases are as fatal as Ebola or the Spanish Flu, so societies hope for treatment and recovery. Early intervention can save lives. In the case of rabies, early vaccination can completely prevent infection of a disease that is otherwise 100% fatal. Public awareness about a disease leads to earlier diagnoses and efforts to seek recovery. But before public awareness, the medical profession field first needs to identify that such a disease even exists. It took almost 80 years after the first person contracted HIV before its “discovery”.
Continued investment in scientific research institutions enables the discovery of vaccines and cures that prevent transmission and increase treatment rates. AZT, the first truly effective drug that prolonged the lives of HIV patients, was developed in partnership between National Cancer Institute (a U.S. government organization) and a pharmaceutical company. The big data revolution also brings hope of a digital epidemiology movement where epidemics can be predicted before they happen.
Society’s Role
By definition, an epidemic is a widespread transmission of an infectious disease across a community. Thus, the entire community plays a role.
Governments coordinate information, track down the movement of diseases, and communicate action plans to the public. The World Health Organization has criticized Liberia’s response to the 2013 Ebola outbreak for having “inadequate” measures to control infections, weak data management, and “weak leadership and coordination.” The SARS outbreak of 2003 may have been contained within Chinese borders had the government not initially suppressed knowledge of the virus. Instead, the virus spread worldwide.
Governments can coordinate large-scale efforts to control the flow of people. Upon learning that SARS had entered its borders, the Singaporean government acted swiftly – they quarantined 8,000 people in their homes and placed another 4,000 cases under telephone surveillance.
The public also needs to have accurate information about best practices to prevent infection. In the 1300s, uninformed individuals tried to end the Black Death by burning scapegoats at the stake and self-flagellation, practices that were ultimately ineffective. Today, healthcare professionals have adopted practices such as vaccinations, the sterilization of needles, and the use of protective gear.
When undertaking these measures, one should remember that responding to an outbreak makes for an ethical minefield. Hollywood has done an excellent job exploring this area. The 2011 film Contagion received praise for realistically depicting some of the moral dilemmas in response to a virus outbreak – the distribution of a limited supply of vaccines, quarantine, forced social distancing, prioritizing access to treatment, using positions of power to serve self interest, and publicity control [4]. And even kitschy thrillers like zombie movies tell moral allegories of how a disrupted society must redefine their definition of family, draw a line between the point of protection vs. attack, and grapple with utilitarian scenarios.
Case Study: HIV
So let’s put together everything we’ve discussed above to look at the spread of HIV over time. The growth of HIV infection looks like a steady growth curve unlike the boom-and-bust of the 1918 Spanish Flu or the exponential growth of the Black Plague.
Infectivity is on the lower end – the virus doesn’t live outside the human body, doesn’t spread through the air, and doesn’t even spread from swapping saliva (unless if you drink gallons of it in one sitting). Bodily fluids must be transmitted into open wounds, so the act of kissing wouldn’t be enough to transmit HIV. Instead, sexual acts with higher likelihoods of tearing and bleeding, such as anal sex, are more dangerous than engaging in vaginal sex.
Contact rates (frequency of risky behavior) depend largely on cultural norms and awareness. In many African countries with high HIV prevalence, sexual education is still a taboo topic and safe sex is not as common. This ignorance leads to misinformed practices that perpetuate the virus, like the belief that having sex with a virgin cures you of HIV. But in countries where discussions about sex is commonplace, adults are expected to get tested and share their results with their sex partners.
HIV prevalence doesn’t experience the same rise and decline behavior of the Spanish Flu because HIV has a relatively long mortality period (10 years without treatment) – long enough that the term “AIDS” (Acquired Immunodeficiency Syndrome) describes just the final stage of HIV infection. Former basketball star Magic Johnson announced that he had contracted HIV in 1991 at the height of his professional career, and to this day has not yet moved into the later stage of AIDS. A mixture of lifestyle habits and taking over 30 drugs each day helps increase his length of life.
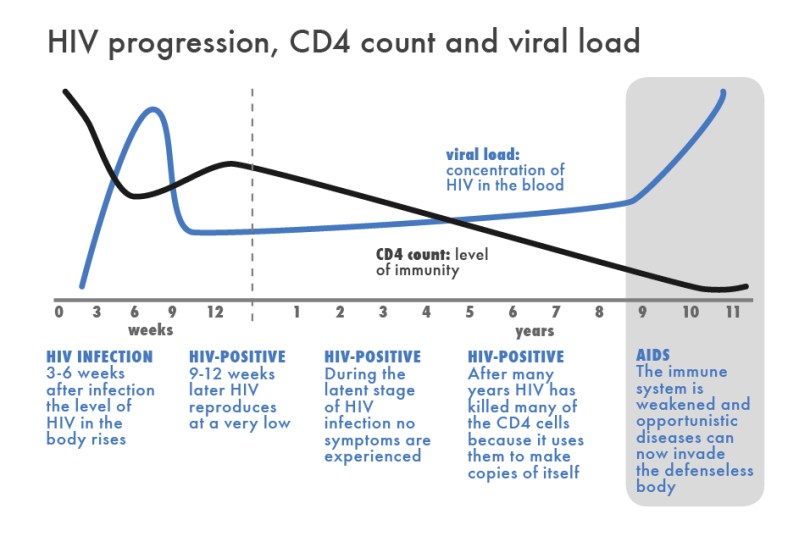
The virus’s initial symptoms are innocuous (flu-like symptoms shortly after infection), and many HIV carriers experience no symptoms until the transition to the AIDS phase years later. So unlike victims of quick-burn epidemics like influenza or Ebola, HIV carriers are largely invisible. Carriers can unknowingly infect other sexual partners over many years, thus increasing the contact rate in our model.
But public education and awareness has improved drastically over the years. Magic Johnson’s retirement announcement challenged incorrect beliefs that HIV only affected gay white men and spurred the public to get tested. In New York City, the number of people seeking HIV tests shot up by 60% within a month. Later that same year, there was such a high demand for tests that people would have to wait for as long as 7 weeks for an appointment.
Public awareness and open communication lines have led to surprising results in the United States – the number of new HIV infections has remained relatively stable over the years despite a growing population base. From 1993 – 1995, AIDS was the top reason for deaths among young Americans between the ages of 25 and 44, peaking at 31,000 deaths in 1995. In 2010, that number dropped down to just 2,600. If other countries adopt similar practices, we may see global HIV prevalence rates fall over time.
By Jonathan Yu and Jenny Zhou
Additional Perusing:
– Play Vax: A game about epidemic prevention
– RadioLab Episode “Patient Zero” – the beginnings of HIV
– RadioLab Episode “Rodney Versus Death” – the case of Rabies patient Jeanna Giese and her unconventional treatment
– China Syndrome by Karl Taro Greenfeld – great on-the-ground reporting of the 2003 SARS crisis all the back to Patient Zero
– The Great Mortality by John Kelly – a very intimate portrait of the Black Death backed by first-hand accounts and impressive amounts of data
+++++
Footnotes
[1] Each player gets to adopt a role that comes with special privileges. The quarantine specialist helps mitigate the infection rate. The medic increases the treatment rate. The scientist speeds up the cure rate. These role cards end up dictating each player’s actions so that collectively, you behave in a way such that treatment rates exceed infection rates. The game is over when the cures to all four diseases have been discovered through the game’s mechanics. With that said I have yet to win this game without bending the rules.
[2] Epidemic refers to the heightened occurrence of people contracting a particular disease, above what is usually expected. These are usually caused by a change in ecology, a genetic change to the parasite population, or the introduction of a new parasite to a particular host population.A pandemic refers to an epidemic that has spread to multiple geographic regions.
[3] HIV is believed to be an evolution of SIV, a virus that infects wild chimpanzees. Humans participating in bushmeat activities commonly acquire SIV.
[4] Director Steven Soderbergh consulted with authorities from the World Health Organization (WHO) and Center for Disease Control (CDC) in order to accurately depict a pandemic’s effect on society. The film was inspired by recent pandemics such as the 2003 SARS epidemic and the 2009 flu pandemic.

{kind=link}
One comment